What is hip dysplasia?
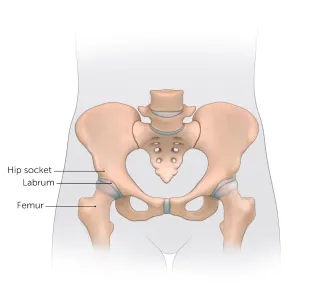
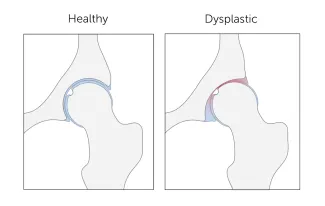
The hip is a ball-and-socket joint. Normally, the ball at the top of the thigh bone fits into the hip socket. Hip dysplasia occurs when the hip joint has not developed properly and the socket (acetabulum) is too shallow. This allows the ball (femoral head) to slip partially or completely out of the joint. Hip dysplasia ranges from a mild abnormality to a complete dislocation of the hip.
Severe cases of hip dysplasia are usually diagnosed during a routine screening within the first few months of a baby’s life. Other times, the problem may only become noticeable as a child grows and becomes more active.
Hip dysplasia is a treatable condition. However, if left untreated, it can cause irreversible damage that will cause pain and loss of function later in life. It is the leading cause of early arthritis of the hip before the age of 60. The severity of the condition and catching it late increase the risk of arthritis. Therefore, monitoring and early intervention are both important to reduce a child’s risk of pain and disability in adulthood.
Who is affected?
Hip dysplasia can affect anyone at any age. Although it is believed to develop around birth, a child with mild dysplasia may not have symptoms for years, or even decades.
- Hip dysplasia in babies is known as infant developmental dysplasia of the hip (DDH).
- When diagnosed in adolescents and young adults, it is sometimes called acetabular dysplasia.
The age at which older kids and young adults with hip dysplasia begin to notice symptoms depend on the severity of the condition and their activity level. Athletes who place a lot of load on their hips by participating in dance, hockey, football, soccer, or track and field may experience symptoms sooner.

Meet Jenna
Hip dysplasia made it difficult for this medal-winning runner and soccer player to lift her leg without searing pain. Today, her athleticism has gained the attention of college recruiters.
Girls and women are two to four times more likely than boys to have hip dysplasia. It also tends to affect first-born children and those who have a close family member with hip problems. Some people with hip dysplasia are affected in only one hip while others have it in both hips.
In boys, the condition tends to be accompanied by other hip problems. These include acetabular retroversion (when the hip socket grows too far over the head of the femur) or CAM lesions (extra bone growth on the surface of the bone that causes extra friction and joint damage).
Hip dysplasia is sometimes confused with hip impingement, which occurs when extra bone grow on the acetabulum or femoral head. The irregular shape creates friction within the joint and wears down cartilage. Some patients have both conditions, both of which cause hip pain and are easy to confuse. However, they are different issues that require different treatments.
Generally speaking, treating hip dysplasia as early as possible can minimize joint damage and reduce the chance of early onset arthritis.
Hip Dysplasia | Hip Dysplasia in Adolescents
What is hip dysplasia in adolescents?
Hip dysplasia occurs when the hip socket (acetabulum) doesn't develop properly and is too shallow to cover the head of the thigh bone (femoral head) completely. Many adolescents and young adults with the condition were born with developmental dysplasia of the hip (DDH). In others, previously healthy hips did not develop properly as their bones and bodies grew.

Meet Louise
Undiagnosed hip dysplasia caused such severe knee pain, this former track star sometimes had trouble walking after competitions. With surgery behind her, and a degree in medicine in the works, she has returned to the sport she loves.
The condition ranges from a mild abnormality of the hip socket to a complete dislocation of the hip. As children become more active and demand more of their legs, the ill-fitting hip joint becomes unstable. The instability damages cartilage inside the joint that becomes increasingly painful over time.
It is important not to ignore hip pain. Hip dysplasia is a treatable condition but early diagnosis and treatment are critical to preventing irreversible damage.
What are the symptoms of hip dysplasia in adolescents and young adults?
Teens or young adults may develop a limp or have hip pain in the front of the hip or groin. For others, the first sign is knee pain. You might hear a clicking sound in your hip. As the damage progresses, you may find it more and more painful to participate in sports and other activities. Without treatment, the pain will continue to become worse.
What causes hip dysplasia in adolescents and young adults?
Some teens and young adults are born with mild DDH that becomes symptomatic as they grow. However, the hip joint continues to develop throughout the teen years and sometimes does not develop properly, even if you were not born with DDH. Doctors are not sure why this happens but they do know that the condition affects girls two to four times as often as boys. People with a close relative with hip problems are also at higher risk.
How is hip dysplasia diagnosed in adolescents and young adults?
Doctors typically use variety of tests to determine if dysplasia is the source of hip pain in adolescents and young adults.
The first step is a thorough patient history and physical exam. The doctor will check your hip for range of motion. They may order imaging studies such as an x-ray, MRI, or CT scan to confirm the diagnosis. Ultrasound-guided diagnostic injection can help your doctor determine the location of your hip pain with greater precision.
How is hip dysplasia treated in adolescents and young adults?
The goal of treatment is to restore normal hip function and eliminate pain. Your treatment will depend on the severity of your condition.
Non-surgical treatment options for adolescents and young adults
Mild to moderate cases of hip dysplasia are often treated with physical therapy and nonsteroidal anti-inflammatory drugs (NSAIDs). If you continue to be in pain after these treatments, your physician may suggest surgery.
Surgical options for adolescents and young adults
Periacetabular osteotomy (PAO) is the main surgical treatment for adolescents and young adults with hip dysplasia. PAO may serve as a lifelong treatment if performed before serious damage occurs within the joint.
The goals of PAO are to:
- reduce or eliminate pain
- maximize the function of your hip
- enable you to return to sport or other activity
Hip Dysplasia | Hip Dysplasia in Babies
What is hip dysplasia in babies?
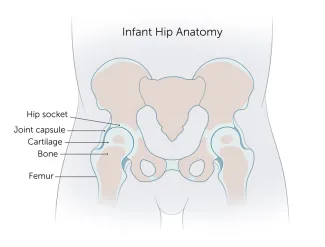
Hip dysplasia in babies, also known as developmental dysplasia of the hip (DDH), occurs when a baby’s hip socket (acetabulum) is too shallow to cover the head of the thighbone (femoral head) to fit properly. DDH ranges in severity. Some babies have a minor looseness in one or both of their hip joints. For other babies, the ball easily comes completely out of the socket.
What are the symptoms of hip dysplasia in babies?
Many babies with DDH are diagnosed during their first few months of life.
Common symptoms of DDH in infants may include:
- The leg on the side of the affected hip may appear shorter.
- The folds in the skin of the thigh or buttocks may appear uneven.
- There may be a popping sensation with movement of the hip.
What causes hip dysplasia in babies?
The exact cause is unknown, but doctors believe several factors increase a child’s risk of hip dysplasia:
- a family history of DDH in a parent or other close relative
- gender — girls are two to four times more likely to have the condition
- first-born babies, whose fit in the uterus is tighter than in later babies
- breech position during pregnancy
- tight swaddling with legs extended
Breech position: Babies whose bottoms are below their heads while their mother is pregnant with them often end up with one or both legs extended in a partially straight position rather than folded in a fetal position. Unfortunately, this position can prevent a developing baby’s hip socket from developing properly.
Tight swaddling: Wrapping a baby’s legs in a straight position may interfere with healthy development of the joint. If you swaddle your baby, you can wrap their arms and torso snugly, but be sure to leave room for their legs to bend and move.

Angela's story
Angela was 5 when her parents brought her to Boston Children’s Hospital, where she was diagnosed with hip dysplasia in both hips.
How is hip dysplasia diagnosed?
Infants in the U.S. are routinely screened for hip dysplasia. During the exam, the doctor will ask about your child’s history, including their position during pregnancy. They’ll also ask if there is any history of hip problems on either parent’s side.
The doctor will do a physical exam and order diagnostic tests to get detailed images of your child’s hip. Typical tests can include:
- Ultrasound (sonogram): Ultrasound uses high-frequency sound waves to create pictures of the femoral head (ball) and the acetabulum (socket). It is the preferred way to diagnose hip dysplasia in babies up to 6 months of age.
- X-ray: After a child is 6 months old and bone starts to form on the head of the femur, x-rays are more reliable than ultrasounds.
How is hip dysplasia treated?
Your child’s treatment will depend on the severity of their condition. The goal of treatment is to restore normal hip function by correcting the position or structure of the joint.
Non-surgical treatment options
Observation
If your child is 3 months or younger and their hip is reasonably stable, their doctor may observe the acetabulum and femoral head as they develop. There’s a good possibility the joint will form normally on its own as your child grows.
Pavlik harness
If your child’s hip is unstable or sufficiently shallow, their doctor may recommend a Pavlik harness. The Pavlik harness is used on babies up to four months old to hold their hip in place while allowing their legs some movement. The baby usually wears the harness all day and night until their hip is stable and an ultrasound shows their hip is developing normally. Typically, this takes about eight to 12 weeks. Your child’s doctor will tell you how many hours a day your child should wear the harness. Typically, children wear the harness 24 hours a day.
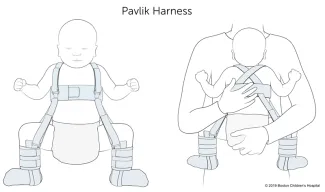
While your child is wearing the harness, their doctor will frequently examine the hip and use imaging tests to monitor its development. After successful treatment, your child will need to continue to see the doctor regularly for the next few years to monitor the development and growth of their hip joint.
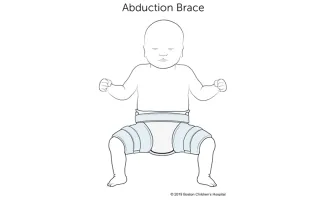
Typically, infants’ hips are successfully treated with the Pavlik harness. But some babies’ hips continue to be partially or completely dislocated. If this is the case, your child’s doctor may recommend another type of brace called an abduction brace. The abduction brace is made of lightweight material that supports your child’s hips and pelvis. If your child’s hip becomes stable with an abduction brace, they will wear the brace for about eight to 12 weeks. If the abduction brace does not stabilize the hip, your child may need surgery.
Surgical treatment options for babies
Closed reduction
 If your child’s hip continues to be partially or completely dislocated despite the use of the Pavlik harness and bracing, they may need surgery. Under anesthesia, the doctor will insert a very fine needle in the baby’s hip and inject contrast so they can clearly view the ball and the socket. This test is called an arthrogram.
If your child’s hip continues to be partially or completely dislocated despite the use of the Pavlik harness and bracing, they may need surgery. Under anesthesia, the doctor will insert a very fine needle in the baby’s hip and inject contrast so they can clearly view the ball and the socket. This test is called an arthrogram.
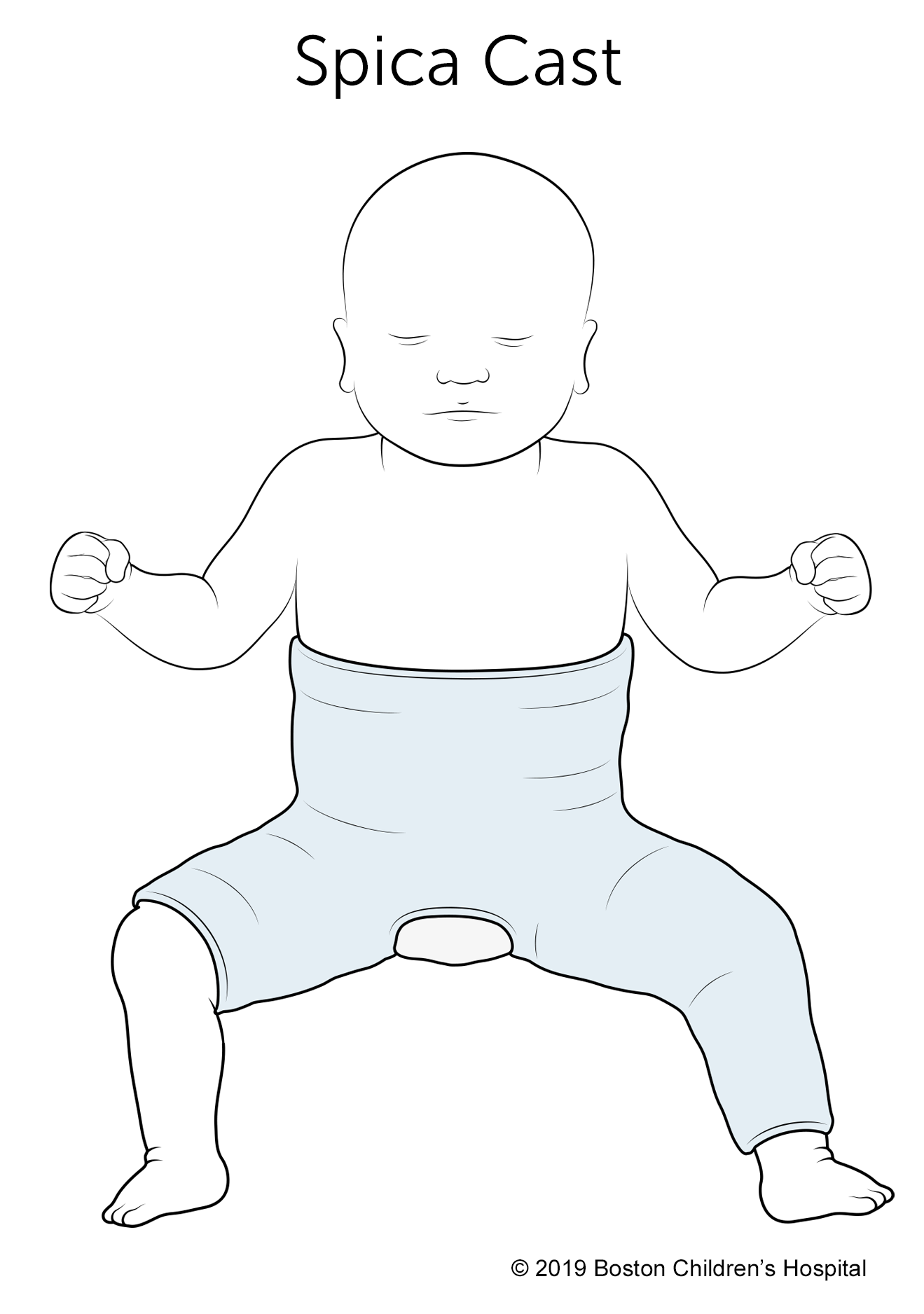
The process of setting the ball back into the socket after the arthrogram is known as a closed reduction. Once the hip is set in place, technicians will put your child in a spica cast. This cast extends from slightly below the armpits to the legs and holds the hip in place. Different casts cover differing amounts of the child’s legs, based on the condition of their hips. Children typically wear a spica cast for three to six months. The cast will be changed from time to time as your baby grows.
Open reduction
If a closed reduction does not work, your child’s doctor may recommend open-reduction surgery. For this, the surgeon makes an incision and repositions the hip so it can grow and function normally. The specifics of the procedure depend on your child’s condition but it may include reshaping the hip socket, redirecting the femoral head, or repairing a dislocation. After the surgery, your child will need to wear a spica cast while they heal.
Follow-up care
Any infant treated surgically for hip dysplasia must be followed periodically by an orthopedist until they have reached physical maturity. At regular visits, their orthopedic doctor will monitor their hip to ensure it develops normally as they grow. Diagnosing and treating any new abnormality early will increase the chance your child will grow up to be active free from hip pain throughout their childhood, the teen years, and adulthood.
Will treatment affect my child’s ability to walk?
Depending on their age during treatment, your child may start walking later than other kids. However, after successful treatment, children typically start walking as well as other kids. By contrast, children with untreated hip dysplasia often start walking later, and many walk with a limp.
How we care for hip dysplasia
The Child and Young Adult Hip Preservation Program at Boston Children’s Hospital is at the forefront of research and innovation. We combine specialized expertise in non-surgical and surgical treatments with structured physical therapy to help children, adolescents, and young adults live healthy, active lives.
Our team has treated thousands of children with every level of complexity and severity of hip deformity. Our hip specialists have pioneered minimally invasive procedures as well as open surgical techniques to help treat patients of all ages. We perform more periacetabular osteotomy (PAO) procedures every year than any other hospital in the country and have helped hundreds of athletes return to the activities they love.
We have the experience to treat you or your child. Our goal is the same as yours: to help you get better so you can return to being healthy and pain-free.
Patient resources
Download these fact sheets to learn more about hip dysplasia and treatment options.
- fact sheet: developmental dysplasia of the hip (DDH)
- fact sheet: Pavlik harness
- fact sheet: hip dysplasia in adolescents and young adults

