Radial Longitudinal Deficiency | Symptoms & Causes
What are the symptoms of radial longitudinal deficiency?
If your child has a mild form of radial longitudinal deficiency, the condition will probably not cause problems with their development or hand movement.
If your child has a severe form, they may have problems moving their hand, fingers, and elbow. Their entire arm will be shorter, with a curved forearm and stiff elbow and fingers. They may also have a small or missing thumb.
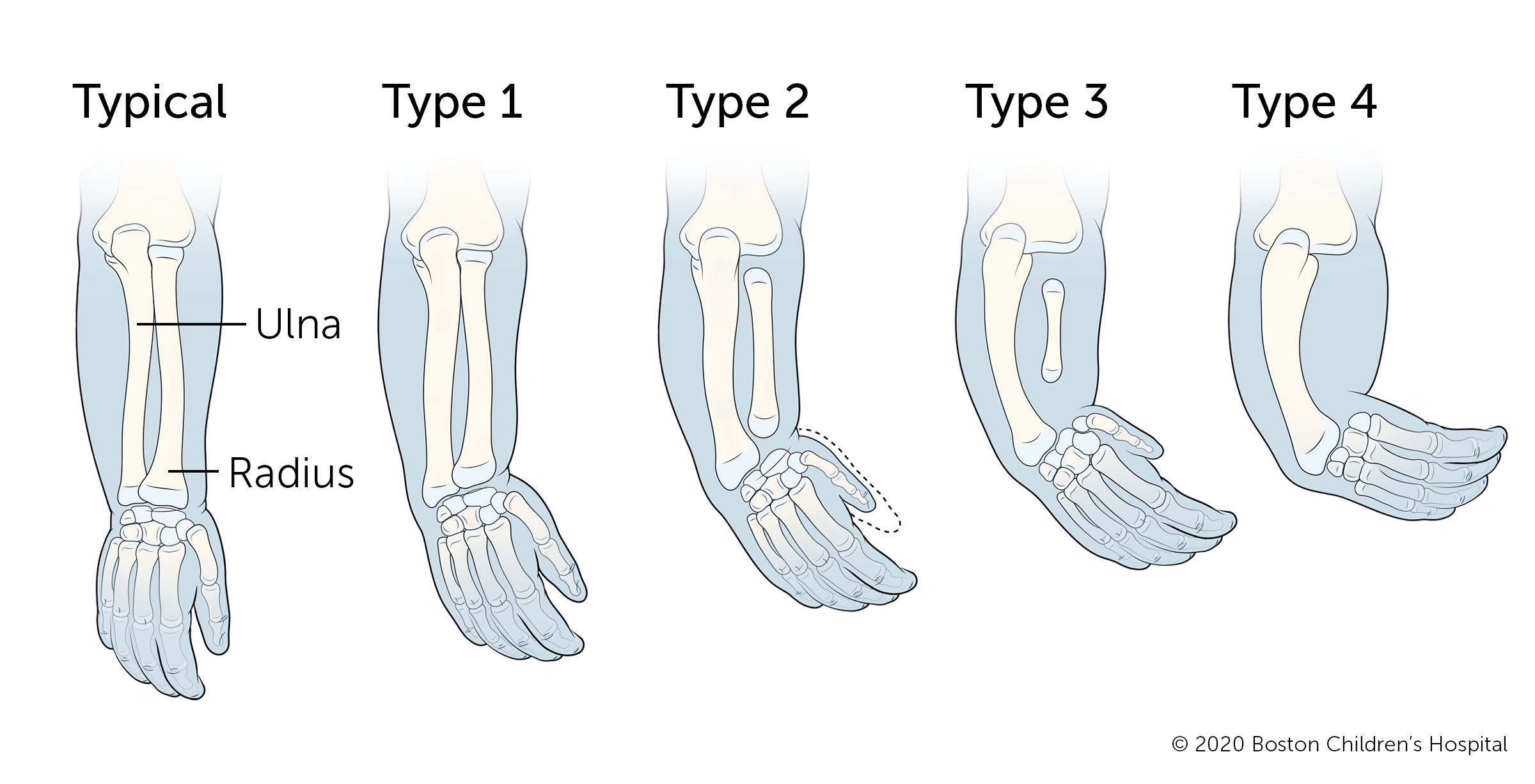
Types of radial longitudinal deficiency
- Children with type 1 radial longitudinal deficiency can move their hand normally. They usually do not need surgery unless it is necessary to correct an underdeveloped thumb.
- In children with type 2 radial longitudinal deficiency, the wrist bends inward, and the ulna bows out. Children with this type often have an underdeveloped thumb.
- Children with type 3 radial longitudinal deficiency are missing most of the radius bone. The wrist bends inward more severely and the hand has limited support. The ulna is bowed. Most children with this type of radial longitudinal deficiency have an underdeveloped or missing thumb.
- Type 4 radial longitudinal deficiency is the most common and most severe form of radial longitudinal deficiency. Children with this type are missing the radius bone and have significant shortness in the forearm. They may also have limited range of motion in their elbow. Most children with type 4 have an underdeveloped or missing thumb, and may have differences in their other fingers as well. Many children adapt by using their pinky finger to pick up toys and other objects.
What causes radial longitudinal deficiency?
Radial longitudinal deficiency usually occurs by chance, although for some people it can also run in the family. Doctors and scientists do not know why some children are born with this condition. There are several theories, including compression of the uterus and blood vessel injury. None of these theories have been proven, however.
There are no known links between this condition and the mother’s lifestyle or anything the mother may do during pregnancy.
Radial longitudinal deficiency is associated with several congenital syndromes, including those affecting the heart, digestive system, and kidneys. It has also been linked to some chromosomal abnormalities, including Down syndrome and Trisomy 18 and 13.
Radial Longitudinal Deficiency | Diagnosis & Treatments
How is radial longitudinal deficiency diagnosed?
Radial longitudinal deficiency is sometimes picked up on a prenatal ultrasound, but the condition cannot be treated until after your baby is born.
If your child’s condition is detected after birth, a doctor will examine their forearm and take an X-ray. Your child’s doctor will check for other differences or syndromes that are associated with radius deficiency. Additional tests could include blood tests and ultrasounds of the kidneys and possibly the heart.
How is radial longitudinal deficiency treated?
Your child’s treatment will depend on how severely their arm and hand are affected. The goals of treatment are to:
- Correct the position of the wrist
- Increase wrist and finger mobility
- Improve hand function
- Preserve growth of the forearm
- Improve the appearance of the hand and forearm
Exercises and splinting
When your child is an infant, their doctor will talk to you about how to perform gentle stretching exercises for your child’s wrist and elbow to help improve the range of motion in those joints.
Even if your child will eventually need surgery, range-of-motion exercises are extremely important. Any improvement in range of motion achieved through exercise will make surgery more effective and possibly less complex. Your baby will probably need to wear a splint at night throughout infancy and during times when they grow quickly.
If your child’s condition is severe, they may wear a cast or splint to gradually stretch the soft tissues in their forearm.
Types of surgery for radial longitudinal deficiency
Your child’s doctor must weigh the decision to perform surgery against any other medical conditions your child may have, as well as the overall function of their arm.
If your baby has severe radial longitudinal deficiency, they may need surgery after a period of stretching and splinting. Surgery is also an option if problems with the thumb interfere with your child’s use of their hand.
Each part of the arm is treated during separate surgeries that may take place over months or years, typically starting when your child is about 1. Below are surgeries your child may need to treat different parts of their arm and hand. The number and timing of these surgeries will depend on your child and their condition:
Wrist surgery
- Lengthening takes place before surgery to gently stretch the hand into a straighter position. A frame is surgically placed on the hand and forearm so that pins go through the ulna and hand. The pins are slowly pushed apart. This may be recommended while your child is an infant if their wrist is tight and hard to stretch. It is also used when a child is older and has another deformity or significant shortening of the forearm.
- Centralization involves repositioning the wrist so the hand sits straight on the end of the ulna. At the time of surgery, surgeons place a pin through the wrist and the ulna. This may stay in place for a year or more after surgery until the ulna broadens and becomes a more stable platform for the wrist.
- Bilobed flap or soft tissue centralization involves repositioning the soft tissues (skin and muscles/tendons) to improve the motion of the wrist. There is no surgery on the bones, as there would be in a formal centralization.
- Splinting is usually necessary both before and after bone or soft-tissue centralization.
Forearm surgery
Osteotomy involves cutting a bone into wedges and reshaping it. In cases of radial longitudinal deficiency, the surgeon will perform an osteotomy on the forearm bones in order to straighten them. The wedges of bone are held in place by pins while the bone heals. These pins are removed once the bone has grown strong in its new position.
Thumb surgery
Many children with radial longitudinal deficiency need surgery to reconstruct their thumb. If the thumb is only mildly underdeveloped, a surgical procedure called an opponensplasty can strengthen the thumb muscles. When the thumb is more significantly underdeveloped or missing, the surgeon may perform a pollicization to reposition the index finger as a thumb.
Elbow surgery
Elbow surgery is rarely needed. Some children who have difficulty bending their elbow will undergo a procedure to release tight soft tissues at the back of the elbow that make the elbow stiff. This can be done separately or in combination with procedures to correct the wrist and thumb.
What is the long-term outlook for radial longitudinal deficiency?
Your child’s long-term outlook depends on the severity of their condition and whether they have any associated conditions.
If your child has a mild case of radial longitudinal deficiency, they will need physical therapy as they grow in order to keep their arm and wrist aligned and strong. They may have minor problems moving and using their arm.
If your child has more severe radial longitudinal deficiency, their arm will have limited range of motion, strength, and movement, but there are many possible ways to adapt. Ongoing physical and occupational therapy are often helpful to help your child get the most use of their arm possible as they grow and develop.
How we care for radial longitudinal deficiency at Boston Children’s Hospital
The Orthopedics and Sports Medicine Department’s Hand and Orthopedic Upper Extremity Program and our the Department of Plastic and Oral Surgery’s Hand and Reconstructive Microsurgery Program have treated thousands of babies and children with radial longitudinal deficiency and other hand problems. We are experienced treating conditions that range from routine to highly complex and can provide your child with expert diagnosis, treatment, and care. We also offer the benefits of some of the most advanced clinical and scientific research in the world.
Our Orthopedics and Sports Medicine Department is nationally known as the preeminent center for the care of children and young adults with a wide range of developmental, congenital, neuromuscular, sports-related, traumatic, and post-traumatic problems of the musculoskeletal system.
Our Department of Plastic and Oral Surgery is one of the largest and most experienced pediatric plastic and oral surgery centers anywhere in the world. We provide comprehensive care and treatment for a wide variety of congenital and acquired conditions, including hand deformities.

